Article
Managing behavioural and psychological symptoms in dementia
- Stephen Macfarlane, Daniel O’Connor
- Aust Prescr 2016;39:123-5
- 1 August 2016
- DOI: 10.18773/austprescr.2016.052
Most patients with dementia have some behavioural and psychological symptoms. While aggression and agitation are easily recognised, symptoms such as apathy may be overlooked.
Behavioural and psychological symptoms should be managed without drugs whenever possible. Although there is little evidence to support their use, antipsychotic drugs are often prescribed to people with dementia.
Before prescribing it is important to exclude other causes of altered behaviour, such as pain or infection. Some symptoms may be artefacts of memory loss rather than psychosis.
Patients with dementia who are prescribed antipsychotic drugs have an increased risk of falls, hospitalisation and death. They should be regularly monitored for adverse effects.
If the patient’s symptoms resolve with drug treatment, reduce the dose after two or three months. Stop the drug if the symptoms do not return.
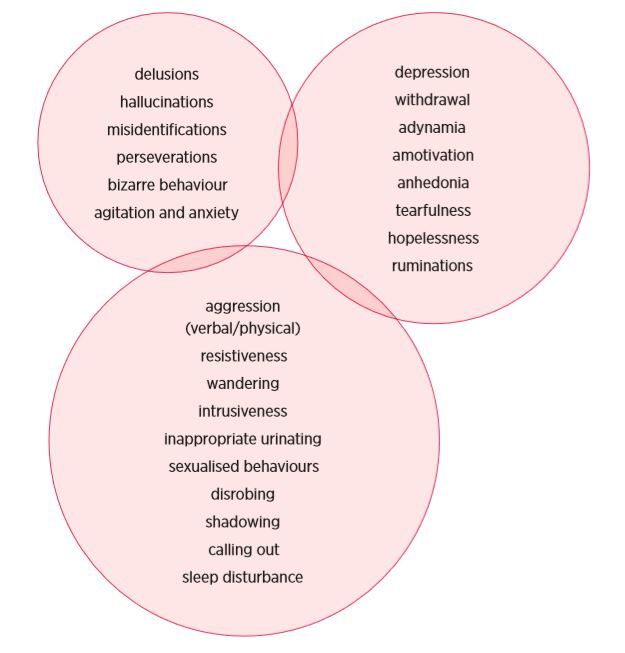
Despite their frequency, certain symptoms are under‑recognised, as their occurrence does not necessarily impinge on the provision of care to the person with dementia. Behaviours that are likely to be missed by care staff are those within the depression cluster (see Fig.). This is because few if any externalising behaviours result, despite the distress experienced by the person with dementia. Behaviours that are harder to ignore are aggression, agitation and psychosis.
General practitioners often find themselves under immense pressure to prescribe. The majority of carers within residential aged-care facilities receive minimal training (a Certificate III in Aged Care can be completed in as little as two days per week over 13 weeks), have a significant and stressful workload, and are paid at a level that is not commensurate with the demands of their jobs. Talking to poorly paid and poorly motivated staff about a complex behavioural intervention that must be implemented consistently across three shifts of carers over the seven-day week is often an exercise in frustration for all parties. Carers, when faced with a behaviour of concern, will often look to the treating doctor for a ‘quick fix’ that is too often reflected in pressure to prescribe.
A number of key principles should guide the management of behavioural and psychological symptoms of dementia. Drugs should only be used when behavioural interventions have failed. They are a treatment of last resort in most cases. Unfortunately, this advice does not seem to be mirrored by prescribing data in Australia. While only about 3% of mental health-related services subsidised by the Medicare Benefits Scheme were provided to those aged 75 and above, over 30% of those within that age group are prescribed psychotropic drugs subsidised by the Pharmaceutical Benefits Scheme (PBS).2,3
The evidence for the effectiveness of most structured therapies for behavioural and psychological symptoms of dementia is both limited and inconsistent. Methodological difficulties of research in this area have the potential to confound most randomised controlled trials.
A recent meta-analysis failed to support the routine use of reminiscence therapy, simulated presence therapy, validation therapy, acupuncture, aromatherapy or light therapy. There is limited evidence that music therapy, pet therapy and hand massage or touch therapy may have beneficial effects in reducing agitation.4
Structured therapies, however, form only a small part of what might be considered non-drug interventions for behavioural and psychological symptoms. Simple techniques such as distraction, redirection, reassurance and reorientation form the core of behavioural interventions that might be applicable in a nursing home setting, and require little other than staff time in order to implement. The choice of intervention should be individualised to the patient and the behaviours that they exhibit, with particular attention being paid to the triggers for each behaviour (e.g. does the problem behaviour only occur at times of nursing intervention, or at particular times of day?). In situations where greater clarity about the role of behavioural interventions might be required, consideration should be given to referral for assessment by local aged psychiatry services or, indeed, to the national Dementia Behaviour Management Advisory Service (DBMAS).
The Figure shows the variety of symptoms that might be encountered. While a drug might have a PBS indication for treating behavioural disturbances, this does not mean that all symptoms are likely to respond equally well to that drug. There is no drug that will stop people wandering, undressing, urinating inappropriately, shadowing staff or calling out. These are behaviours for which a specific history must be taken in order to elicit and address contributing factors such as pain, infection, and local irritation for which psychotropic drugs have little, if any, role.
Even symptoms such as delusions, which might seem to be suited for drug therapy, can be misleading in cases of dementia. It may be unproductive to think of certain ‘delusions’ as being truly psychotic in nature. Instead it is better to view certain beliefs as artefacts of poor memory. A prime example would be the ‘delusions of theft’ reported in approximately 22% of patients with dementia.5 Other examples could include the failure to correctly identify carers, family members, a spouse, or indeed a patient’s own reflection in the mirror.
The general principles of prescribing for older people also apply to patients with behavioural and psychological problems in dementia:
Many different classes of drugs have been suggested as treatments for behavioural and psychological symptoms of dementia. There is limited evidence for antipsychotics, antidepressants, benzodiazepines, anticonvulsants, hormonal treatments, cholinesterase inhibitors and memantine. For the most part, this evidence is weak and effect sizes for most drugs are small.6 In practice, choices are limited within the PBS. Only risperidone, among the atypical antipsychotics, is subsidised for the treatment of psychotic symptoms and aggression. As of July 2015, this approval has become restricted to patients with Alzheimer’s dementia, with the approved duration of treatment being limited to 12 weeks.7
While the risks of cerebrovascular adverse events associated with antipsychotic drugs in patients with dementia are now well known, benzodiazepines are not a ‘safe’ alternative. They pose additional risks from sedation and higher rates of falls, fractures and death.
All prescribers should be aware that placebo response rates are very high for any drug prescribed for behavioural and psychological symptoms of dementia. This may reflect a component of ‘treating the staff’ by prescribing (anything) within a residential aged-care facility in response to the emergence of a problematic behaviour. Alternatively, the high placebo response rate may reflect the useful aphorism that ‘all symptoms in dementia cure themselves with the passage of time’. The natural history is that the symptoms wax and wane according to both environmental factors and factors related to disease progression. There should thus be no reluctance about a trial of deprescribing within 2–3 months of the behaviour settling. If the symptoms do not re-emerge, stop the drug.
Giving psychotropic drugs to patients with dementia increases the risks of hospitalisation, falls, cerebrovascular adverse events and death. Nursing home patients with dementia who are prescribed antipsychotics are 1.9–2.4 times as likely to have an adverse event that requires hospitalisation, or to die, within 90 days of starting treatment. For patients whose treatment begins in the community the risks are elevated 3.2–3.8 times.8
Drugs are an augmentation to behaviour management, not a replacement for it. Regardless of whether a decision to start pharmacotherapy has been made or not, behavioural management strategies should be continued.
Conflict of interest: none declared
Head of Clinical Governance, Dementia Centre, HammondCare, Sydney
Emeritus professor, Aged Mental Health Research Unit, Monash University, Melbourne
