Article
Managing menopausal symptoms
- Terri Foran
- Aust Prescr 2010;33:171-5
- 1 December 2010
- DOI: 10.18773/austprescr.2010.082
Until the mid 1990s, hormone therapy was seen as not only a safe means of relieving troublesome menopausal symptoms but as a way of preserving youth and vitality. Adverse findings from a number of studies in the 1990s cast doubt on some of the earlier claims, but it was the publication of the Women's Health Initiative study in 2002 that resulted in a complete reappraisal of the principles of menopause management.
Menopause, literally the 'end of menstruation', marks an important transition in a woman's life and occurs in Australia at an average age of 51 years. Menopausal symptoms, which may commence even before the last menstrual period, include vasomotor symptoms, urogenital problems, psychological changes, sleep disturbance and decreased libido. Managing patients with these symptoms can be a challenge.
Vasomotor symptoms include hot flushes, night sweats and formication, which is a particularly unpleasant sensation that feels like ants crawling on the skin. It is estimated that up to 80% of women experience vasomotor symptoms around the time of menopause with an average duration of 5–6 years.1 However, one in four women will still experience significant vasomotor symptoms well into their sixties and in 10% these will persist for life.
Regardless of any other therapies, education and lifestyle advice are integral to effective menopause management. Since smoking has the added impact of increasing the severity of vasomotor symptoms and increasing the risk of osteoporosis,2 menopause provides a good opportunity to discuss smoking cessation.
Dietary modification and the use of herbal supplements are avenues commonly explored by women seeking a more natural approach to menopause management. For some women with milder symptoms, avoidance of known vasomotor triggers such as alcohol, hot drinks and spicy foods may be the only intervention required. Although a diet rich in plant oestrogens such as those found in foods like soy, chickpeas, lentils and flaxseed is likely to be a more healthy option, there is unfortunately no clear evidence that they improve vasomotor symptoms for the majority of women.3
Red clover extract has been widely used for the relief of vasomotor symptoms, but there is no convincing evidence that it is any more effective than placebo. 4, 5A number of small clinical trials investigating other herbal products – such as dong quai, Ginkgo biloba , wild yam and Vitex agnus castus – have also shown no benefit over placebo.
Black cohosh is a herbal compound which appears to have some serotonergic activity. Its use for menopausal symptoms remains controversial, with some studies indicating significant improvement while others have failed to demonstrate any benefit over placebo. Black cohosh preparations vary in dose and potency and this further complicates their evaluation as a treatment. Since at least some reviews indicate evidence for its effectiveness,6 it may be worth trying in those women who are looking for a natural alternative to oestrogen therapy. In my experience it is relatively safe to use and is available as an over-the-counter product. The commonest adverse effect is gastrointestinal upset but there have been reports of idiosyncratic liver failure7 and all black cohosh products marketed in Australia now carry a warning to this effect.
Women using systemic oestrogen therapy can expect a 75% reduction in the frequency of hot flushes and an 87% reduction in their severity.8 However, there are risks associated with hormone therapy. Most of the contemporary evidence is derived from the Women's Health Initiative trial data.9 Although it is the oestrogen which controls menopausal symptoms, women with a uterus also require progestogen for at least 10 days per month to prevent endometrial hyperplasia ( Table 1 ). For such combined therapy there appears to be an increased risk of coronary artery disease, thromboembolism and stroke from the time of initiation. However, some argue that the risk of heart disease is less if therapy is commenced before the age of 60.10,12
Table 1 - Progestogens used in combined therapy for menopausal symptom
| Cyclical therapy | Dydrogesterone 10 mg Medroxyprogesterone 5–10 mg Norethisterone/norethisterone acetate 0.7–2.5 mg |
| Use for at least 10 days per month until 12–18 months after last menses. Allows for scheduled monthly bleed. | |
| Continuous therapy | Dydrogesterone 5 mg Medroxyprogesterone 2.5–5mg Norethisterone/norethisterone acetate 0.35–1 mg |
| Defer until 12–18 months after last menses. No scheduled bleed. | |
| Progestogen intrauterine device | Releases 20 microgram levonorgestrel daily |
* adapted from 'Hormone replacement – oestrogen and progestin dosage schedule'. National Prescribing Service. 2009 Aug. www.nps.org.au/ppr_47_insert [cited 2010 Nov 16]
An increase in cases of breast cancer was also seen after 4–5 years of combined hormone therapy, with eight additional cases per 10 000 women years. Therapy with oestrogen alone appears to be associated with fewer risks, with an increased risk of stroke being the sole adverse finding after seven years.13
A variety of hormonal preparations and different delivery systems are available in Australia. As a general principle the lowest dose of oestrogen should be prescribed that adequately controls symptoms, with the appropriateness of continuing therapy assessed at 6–12 month intervals. Typical starting doses for oestrogen are shown in Table 2, but even at the six-month review it may be worthwhile attempting to reduce the dose further.
Table 2 - Typical starting doses of oestrogens for menopausal symptoms
| Oral |
Conjugated equine oestrogens 0.3–0.625 mg Oestradiol/oestradiol valerate 1–2 mg |
| Transdermal (over 24 hours) |
Oestradiol 25–50 microgram Oestradiol gel 1 mg/g |
| Sub-dermal implant (usually reserved for women who have had a hysterectomy) | Oestradiol 50 mg |
* adapted from 'Hormone replacement – oestrogen and progestin dosage schedule'. National Prescribing Service. 2009 Aug. www.nps.org.au/ppr_47_insert [cited 2010 Nov 16]
Within two months of commencing therapy approximately 80% of women will achieve adequate symptom relief.14 With the remaining 20%, it may be useful to explore an alternative delivery system before increasing the dose. Older women who still require therapy may find their symptoms are controlled on half the standard starting dose.
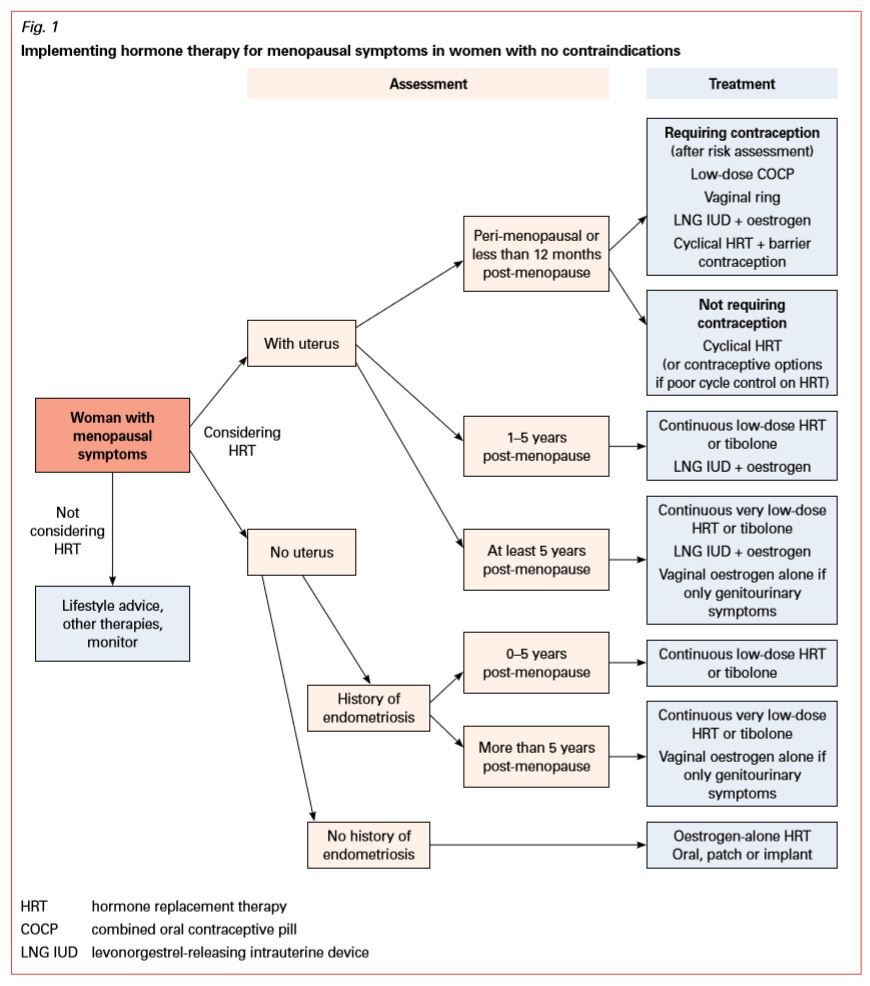
Tibolone is a steroid which has oestrogenic, progestogenic and androgenic activity. The standard dose is 2.5 mg although a half dose could be considered in older patients. Once a decision has been made to commence hormone therapy, the approach to treatment will be influenced by many factors ( Fig. 1 ).
Transdermal progesterone cream has been used for the management of menopausal symptoms since the 1970s. It is minimally absorbed through the skin and there is no good evidence for its usefulness in relieving flushes, or in improving mood, libido or lipid profile.15
When hormone therapy is contraindicated, or when women choose not to use it, low-dose selective serotonin or noradrenaline reuptake inhibitors may be considered. In short-term trials, they have been shown to reduce the number and severity of hot flushes by approximately 60%. 16, 17A quarter to a half of the antidepressant dose is recommended, and in fact higher doses have the potential to make vasomotor symptoms worse. However, adverse effects such as breast tenderness and sexual dysfunction may still limit the use of these drugs in some women even at such low doses. Venlafaxine and paroxetine appear to be the most effective of this class for this purpose. Paroxetine should be avoided in breast cancer survivors on tamoxifen since liver enzyme inhibition may render tamoxifen less effective.18
Clonidine and high-dose progestogens also seem to be effective at reducing troublesome vasomotor symptoms in some women, but adverse effects tend to limit their widespread use. A number of small trials19 have indicated that gabapentin and pregabalin may also be effective in controlling hot flushes, but expense and limited clinical experience has meant that their use is usually restricted to those women with significant symptoms who have failed to respond to other therapies.
Compounded bioidentical hormone therapy has been widely promoted in Australia. These preparations are said to have been derived only from natural products such as wild yam and soy and to deliver steroids identical to those made by the woman's own body. Advocates claim the ability to titrate the preparation to the woman's own individual hormonal needs, guided by salivary or blood tests.
Most compounded preparations deliver a combination of oestriol and oestradiol. Other hormones such as oestrone, progesterone, testosterone and dehydroepiandrosterone may be added.
The hormone therapy is delivered by means of a dissolvable lozenge (troche) or a transdermal cream. There is no doubt that many women find these preparations effectively relieve their menopausal symptoms. The problem is that although bioidentical hormones are often perceived by women as a safer alternative to conventional hormone therapy, there is actually no evidence for this, particularly regarding long-term safety.20 One emerging concern is that the natural progesterone used in many bioidentical regimens to protect the endometrium may not be particularly effective, especially with long-term use. There have been a number of reports recently of endometrial hyperplasia and endometrial cancer in users.21
Unlike vasomotor symptoms, urogenital symptoms such as vaginitis, dyspareunia, cystitis and incontinence tend to worsen as a woman grows older.
Pooled data from several randomised controlled trials indicate that oestrogen improves genital symptoms regardless of the route of administration.22 Vaginal oestrogen is the preferred delivery system for women whose symptoms are primarily urogenital. There is minimal systemic absorption and when vaginal oestrogen is used at the recommended dosages progestogen cover is not necessary in women with a uterus. Even this small absorbed dose may however compromise therapy in breast cancer survivors receiving aromatase inhibitors, such as anastrozole.
Vaginal oestrogen may also be useful in the 27% of women who still experience vaginal symptoms when using low-dose systemic hormone therapy.23 Oestradiol is more potent than oestriol and will therefore provide a more rapid clinical effect when used topically. Vaginal tablets tend to be better tolerated than pessaries and creams since they result in less vaginal discharge. As a therapeutic option vaginal oestrogen remains very much underused, particularly in women troubled by recurrent urinary tract infections and incontinence.
For women who cannot, or do not wish to, use even low-dose vaginal oestrogen, polycarbophil vaginal moisturisers have been shown to improve vaginal pH and normalise vaginal cytology.24
Lubricants can also be useful for augmenting natural lubrication during intercourse. Silicone lubricants offer particular advantages for the older couple since they do not absorb so easily into the skin.
Painful sex is a potent inhibitor of desire and local oestrogen therapy may be all that is required in some women. A recent review of postmenopausal trials indicated that conventional oestrogen hormone therapy tended to increase sexual desire, arousal and satisfaction.25
A gradual decline in androgen levels from the mid-thirties may lead to symptoms such as decreased libido and a lack of energy in some women. Several small studies26 suggest that the androgenic component of tibolone may improve both sexual interest and general well-being. However, the role of androgens in the treatment of postmenopausal loss of libido remains controversial. There are currently no preparations licensed for use in women across Australia, though a low-dose transdermal testosterone cream is available on prescription in Western Australia. Androgen therapy should never be used indiscriminately and only after discussion with the patient about potential adverse effects.
There is also no doubt that study after study has shown that sexual satisfaction is most closely correlated with satisfaction with the relationship. Any pharmacological therapy may be more effective if combined with couple counselling.
The promotion of a healthy lifestyle forms an integral part of an overall approach to menopause management. The findings of the 2002 Women's Health Initiative study profoundly affected long-held notions as to the benefits and safety of menopausal hormone therapy, though it remains a useful option for those with significant symptoms. Vaginal oestrogen therapy in particular provides excellent relief of genitourinary symptoms with very few associated risks. Although many women regard complementary therapies as a safer alternative to conventional medical treatment, there is conflicting evidence as to their effectiveness and long-term safety. The application of an evidence-based approach to decision-making should assist both clinician and patient to make the choices that are most appropriate to a woman's individual needs.
Sexual Health Physician, Lecturer, Taylor Square Private Clinic, Darlinghurst; School of Women's and Children's Health, University of New South Wales, Sydney
