Abnormal laboratory results
Measuring vitamin D
- Paul Glendenning
- Aust Prescr 2015;38:12-15
- 1 February 2015
- DOI: 10.18773/austprescr.2015.004
When assessing vitamin D status, measure serum 25-hydroxyvitamin D concentration as this reflects total body vitamin D reserves.
Recent Australasian guidelines outline who should be tested for vitamin D deficiency, who should be treated and when repeat testing should be performed.
A 25-hydroxyvitamin D threshold of at least 50 nanomol/L at the end of winter is a suitable treatment target. Measurement can be repeated after three months of repletion, and thereafter less frequently unless new risk factors for vitamin D deficiency arise.
When interpreting vitamin D pathology reports, practitioners should be aware that some laboratories quote reference limits which are based on overseas rather than Australian guidelines.
Multiple metabolites of vitamin D are present in the circulation (see Fig.). Vitamin D is synthesised in the skin following ultraviolet B radiation exposure. It can also be obtained from the diet. There are two major circulating forms of vitamin D: 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D. Two steps are involved in the metabolic activation of vitamin D in the body. The second step produces 1,25-dihydroxyvitamin D and occurs in the kidney plus many other body tissues.
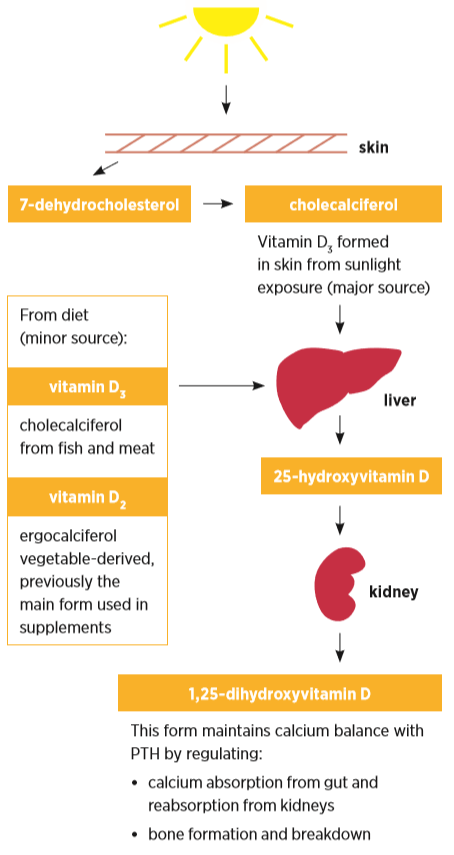
PTH parathyroid hormone
Vitamin D has three main functions:
While 1,25-dihydroxyvitamin D is the functionally active vitamin D metabolite, deficiency is defined according to the measured concentration of circulating 25-hydroxyvitamin D. The serum concentration of 25-hydroxyvitamin D and not 1,25-dihydroxyvitamin D is associated with fracture risk.1 25-hydroxyvitamin D is a good reflection of substrate available for local synthesis of 1,25-dihydroxyvitamin D. Due to diminishing ultraviolet B light exposure, 25-hydroxyvitamin D concentrations decline in winter.
Moderate to severe vitamin D deficiency (25-hydroxyvitamin D <30 nanomol/L) is causally associated with osteomalacia and rickets in children. Mild vitamin D deficiency (25-hydroxyvitamin D <50 nanomol/L) was first associated with hip fracture and subsequently other osteoporotic fractures. Correction of vitamin D deficiency and adequate calcium intake have been cornerstones of osteoporosis management. Most evidence for fracture reduction with current antiresorptive therapies has been from trials where participants were vitamin D and calcium replete, or if not, they were receiving adequate supplementation.
Vitamin D receptor expression has been found in tissues other than bone. Conversion to the active metabolite can be achieved through local enzymatic action. Consequently, vitamin D may exert paracrine or autocrine extra-skeletal effects.3 These effects have generated much research but most studies are observational. Outcomes from these studies have several inherent biases. The major bias is that illness can result in reduced outside activities, diminished sunlight exposure and low 25-hydroxyvitamin D. Low concentrations of 25-hydroxyvitamin D could be a consequence, rather than a cause, of disease. Two recent systematic reviews have concluded there is insufficient evidence to establish a role for vitamin D replacement in extra-skeletal disease. Several large randomised clinical trials in Australia and overseas are planned or underway and may help resolve this issue definitively.4,5
The Royal College of Pathologists of Australasia published a position statement to clarify the role of vitamin D testing in vitamin D deficiency, with guidelines for who should be tested, and when repeat testing should be performed.6 The recommendations, broadly consistent with current evidence, advocate testing in individuals at increased risk of vitamin D deficiency and provide clinical indications for vitamin D measurement (see Box).
Repeat testing is commonly advised, because the nadir of parathyroid hormone suppression following supplementation with cholecalciferol (25-hydroxyvitamin D3) can take at least three months and the response can vary between individuals. Consequently, repeat testing after three months is recommended in most guidelines. In patients already taking long-term replacement (including when combined with other treatments such as a bisphosphonate) or those who have a higher fracture risk, repeat testing annually at the end of winter may be helpful, especially if risk factors for vitamin D deficiency have changed.
Initial methods using liquid chromatography or competitive protein binding were cumbersome and not suited to routine laboratory analysis. Subsequent assays used a simpler extraction method which separated 25-hydroxyvitamin D from its binding protein and allowed quantification of total 25-hydroxyvitamin D using a radio-labelled antibody. However, as test requests increased, this manually intensive method became impractical.
Automated assays use a variety of proprietary reagents to release 25-hydroxyvitamin D from its binding protein, and different antibody detection methods. These methods have been problematic and subject to interference from other antibodies present in the sample. These can cause falsely high results, or suboptimal release of 25-hydroxyvitamin D from its binding protein resulting in falsely low results. Initial automated immunoassays were also not optimally standardised.7
To resolve these limitations, newer assays using liquid chromatography and more specific detectors containing two mass spectrometers were developed. These methods have not been widely adopted as they require expensive hardware and technical expertise. The lack of a reference standard also meant that disagreement between these methods was still a problem.
The US National Institute for Standards and Technology developed separate serum-based standard reference materials to help minimise inter-method disagreement and reduce bias. A reference method using liquid chromatography tandem mass spectrometry measurement from the University of Ghent has been adopted by the US Centers for Disease Control and Prevention. The first vitamin D standardisation certification program administered by the US Centers for Disease Control and Prevention is now in place. More than eight methods have achieved certification in this program including several automated, commercially available immunoassays. To achieve annual certification, tests must have a bias of ±5% (closeness to the true result) and an imprecision (reproducibility) of 10% or less. Consequently, routine immunoassay methods are improving and inter-method disagreement is diminishing as testified in external quality assurance programs, such as the one administered by the Royal College of Pathologists of Australasia and the Australasian Association of Clinical Biochemists. All Australian laboratories providing routine laboratory testing are required to be enrolled in appropriate external quality assurance programs.
Surrogate measures indicate that a 25-hydroxyvitamin D threshold of 50 nanomol/L is a suitable target for treatment. Supplementation of patients at highest risk for fracture should aim to achieve above this target.
No clinical studies investigating the effectiveness of calcium and vitamin D treatment on fracture reduction have recruited people based on their 25-hydroxyvitamin D concentrations. Also, no intervention studies with calcium and vitamin D targeted the 25-hydroxyvitamin D concentration required for fracture prevention. Consequently, the threshold of 50 nanomol/L is determined by surrogate measures which relate fracture risk factors to vitamin D concentrations.
An observational study of American women found hip fractures were more common in women with 25-hydroxyvitamin D concentrations below 47.5 nanomol/L.8
Parathyroid hormone was the first biomarker to indicate that a 25-hydroxyvitamin D threshold of 50 nanomol/L was adequate based on the change in parathyroid hormone with cholecalciferol and calcium therapy.9 This threshold has been verified in a larger study.10
Data using biochemical bone turnover markers show that the 25-hydroxyvitamin D threshold for higher bone resorption and hence higher fracture risk is closer to 50 nanomol/L than to 75 nanomol/L.11
Data from over 1200 community-dwelling men over the age of 65 years found a 25-hydroxyvitamin D below 49 nanomol/L was associated with higher rates of loss of hip bone density.12
The change in serum calcium following oral calcium loading has been used as a surrogate measure of fractional calcium absorption.13 This estimate is less accurate than dual stable isotopic calcium studies which use two calcium isotopes − one isotope is ingested and one is infused to correct for renal and gastrointestinal recycling. A study assessing fractional calcium absorption (using dual stable isotopic calcium) in individuals before and after cholecalciferol supplementation found that absorption was 3% higher when 25-hydroxyvitamin D was above 100 nanomol/L compared to when it was 55 nanomol/L, a negligible difference.14
Practitioners should pay attention to the measured amount of 25-hydroxyvitamin D but be cautious of quoted reference limits reported by some laboratories. The different threshold limits quoted by laboratories are not due to methodological differences, but to differences in the interpretation of data from surrogate measures and to the use of overseas, rather than Australian, guidelines.
Most supplements in Australia provide cholecalciferol 500−1000 IU (vitamin D3) either as a single supplement or combined with calcium. Some clinicians advise a higher dose in patients with severe vitamin D deficiency (25-hydroxyvitamin D <12.5 nanomol/L) compared with less severe forms. A higher dose may also be required in patients taking anticonvulsant drugs, those with obesity or nephrotic syndrome, or following biliopancreatic bypass surgery.
Daily calcium with 800 IU of cholecalciferol was effective at preventing non-vertebral and hip fractures in elderly French women.15 In a West Australian study of hip fractures in patients with vitamin D deficiency, a daily dose of cholecalciferol 1000 IU was sufficient to attain 25-hydroxyvitamin D concentrations greater than 50 nanomol/L in patients adherent to treatment.16
Evidence from an Australian randomised controlled study in 2200 women at high risk of hip fracture has questioned the use of annual high-dose cholecalciferol therapy.17 Risk was based on maternal history of hip fracture, past personal fracture history or self-reported falls. Women receiving oral cholecalciferol 500 000 IU annually experienced 26% more fractures than those receiving placebo. This was attributed to a 31% higher rate of falls in the first three months after dosing. In view of these results, daily, weekly or even monthly vitamin D replacement therapy can probably be safely used, but annual high-dose replacement should be avoided.
Vitamin D is one of the most commonly requested tests. Replacement of vitamin D should be started when circulating levels of 25-hydroxyvitamin D are low (<50 nanomol/L at the end of winter) and when patients are at increased risk of falls or fractures. Annual testing of 25-hydroxyvitamin D at the same laboratory, at the end of winter in patients who are concerned about fracture risk or falls is appropriate management in 2014.
The author has received financial support from MSD, Novartis, Sanofi-Aventis, Servier, Eli Lilly and Amgen for conference attendance.
Consultant endocrinologist and chemical pathologist, Department of Clinical Biochemistry, Royal Perth Hospital, School of Medicine and Pharmacology, University of Western Australia
