Editorial
Quality use of medicines – are we nearly there yet?
- Anthony Smith
- Aust Prescr 2012;35:174-5
- 3 December 2012
- DOI: 10.18773/austprescr.2012.077
In 1992 the Australian Government adopted a policy on the quality use of medicines, or QUM.1 The policy aimed to foster judicious, appropriate, safe and efficacious use of medicines through active partnerships between consumers, health professionals, the pharmaceutical industry and government. It became an important component of our National Medicines Policy (Fig. 1).2
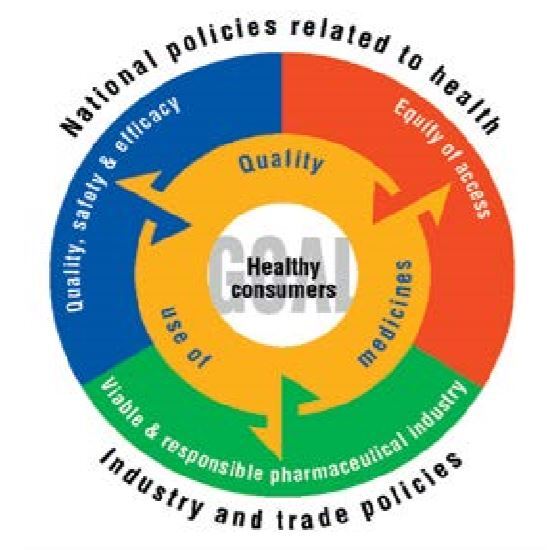
Quality, safety and efficacy are regulated by the Therapeutic Goods Administration, equity of access is achieved through the Pharmaceutical Benefits Scheme, while the pharmaceutical industry provides the medicines we use. Quality use of medicines links all of these to the central objective of improving the health of all Australian consumers.
Much has been accomplished in 20 years. For example, the government funded the National Prescribing Service (NPS) in 1998 as the principal organisation working towards QUM. The NPS, now known as NPS MedicineWise, has an independent board of directors, but is also charged with generating savings for the Pharmaceutical Benefits Scheme as a condition of continued funding. Not surprisingly therefore, NPS MedicineWise has needed to address topics which were clinically important, but also had the capacity to yield savings. Antibiotics were an early (and continuing) target as overuse and misuse promote antimicrobial resistance, create adverse events and generate unnecessary costs.
NPS MedicineWise promotes QUM through a range of activities. These include the educational visiting program to doctors through general practice networks, the National Prescribing Curriculum (now being used by senior students in almost all medical schools), the provision of objective information to health professionals, plus publications and telephone ‘hotlines’ for consumers. The newer ‘Be medicinewise’ program addresses consumer education with a special focus on older people, who have the largest medication burden.
The reach of these and other programs has increased over the years. The latest evaluation report shows 57% (13 774) of the general practitioner workforce participated in NPS MedicineWise activities in 2010–11.3 However, relatively little attention has been given to hospitals, despite the great influence of opinion leaders such as hospital specialists on the prescribing of junior doctors and general practitioners.4
Meanwhile state and territory governments are building their own QUM programs and their expert advisors recently came together to form the national Council of Australian Therapeutic Advisory Groups.5 Many general practice organisations have QUM programs. The special needs of indigenous communities are also being addressed.6
Supporting information for QUM comes from many sources. These include Australia’s own national formulary (the Australian Medicines Handbook) and evidence-based guidelines such as those produced by Therapeutic Guidelines Ltd.
The QUMmap, a valuable database of initiatives across Australia, shows the breadth of activity in QUM.7 Clearly the concepts and many of the tools of QUM have permeated widely in our health system.
What of outcomes? We have to accept that exemplary QUM will not necessarily improve all health outcomes. For most chronic non-communicable diseases that are at the forefront of public health concerns, factors other than medicines (exercise, diet, stopping smoking) play a big role. It is difficult but not impossible to disentangle all the influences and their quantitative contributions to achieving better health. As Professor Mant wrote at the end of the first 10 years of our QUM policy, ‘A key research question will be whether better use of medicines achieves better health outcomes’.8 This question remains unanswered for most diseases.
Not yet tackled is the quality use of complementary medicines. It is difficult to define quality use for a product whose efficacy has not been demonstrated. Under current regulations, sponsors of listed complementary products which are not making high level claims (for example to treat, modify or prevent serious illness) are required to ‘hold the evidence’ for whatever they claim. This evidence is not scrutinised unless there is a postmarketing review or the product is the subject of a challenge through the Therapeutic Goods Administration. Consumers also have a right to evidence-based information about these products.
How then shall we know when we are ‘nearly there’ with QUM? Maybe when we have:
Professor Smith is the former Chair of the Pharmaceutical Health and Rational Use of Medicines Committee and former Chair of the Advisory Committee on Complementary Medicines. He was also a member of the board of the National Prescribing Service.
Professor Emeritus, Clinical Pharmacology, Calvary Mater Hospital, Newcastle, New South Wales
