Diagnostic tests
Testing for coeliac disease
- Diana Lewis, James Haridy, Evan D Newnham
- Aust Prescr 2017;40:105-8
- 1 June 2017
- DOI: 10.18773/austprescr.2017.029
Coeliac disease is an immune-mediated condition in which the intestinal mucosa is damaged by exposure to gluten.
Up to 50% of people with coeliac disease are asymptomatic. A high index of suspicion is therefore required especially in at-risk groups.
Serological investigation alone is insufficient to make the diagnosis. Up to 5% of patients with coeliac disease can have negative serology.
Genotype testing for coeliac disease is most useful in the exclusion of coeliac disease. A positive test does not confirm the diagnosis.
Definitive diagnosis requires gastroscopy and duodenal biopsy. An empirical trial of a gluten-free diet has no role in the diagnosis of coeliac disease.
Coeliac disease is an immune-mediated condition that occurs in people who are genetically susceptible. There is an abnormal response to dietary gluten resulting in inflammation and damage to the small bowel mucosa. Approximately 1 in 70 Australians have coeliac disease, however it is suspected that only 20% of people with the disease are diagnosed.1 Typical symptoms include fatigue, diarrhoea and weight loss, but up to 50% of patients with coeliac disease are asymptomatic.2 Untreated coeliac disease can lead to complications that include early onset osteoporosis, nutrient deficiencies, infertility and malignancy. The only currently available treatment for coeliac disease is a lifelong, strict gluten-free diet.
The toxic proteins that cause coeliac disease are derived from gluten present in wheat, rye, barley and oats. They induce an immune response that results in the typical histological features of coeliac disease. These include loss of the intestinal villi (villous atrophy) and histological evidence of inflammation (crypt hyperplasia and intraepithelial lymphocytosis). The immune response produces circulating antibodies that can be measured in the serum. More than 99% of patients with coeliac disease have a genetic predisposition in the human leukocyte antigen HLA-DQ2 and DQ8. Importantly, approximately half of the Australian population carry the genes, so they are not markers for coeliac disease.
There continues to be uncertainty about oats which contain the protein avenin (a gluten protein) which can cause small bowel mucosal damage in some people with coeliac disease. Complicating this issue is that oats are commonly processed in the same environment as wheat-containing products with the consequent risk of cross-contamination. Based on current recommendations, oats should not be consumed on a gluten-free diet.
Non-coeliac gluten sensitivity is a separate clinical entity. It describes the patients who report gastrointestinal symptoms that improve on exclusion of gluten from the diet but who have no demonstrable small bowel mucosal damage when exposed to gluten. The likely cause of these symptoms is that most foods that contain gluten also contain fermentable carbohydrates such as fructans. Fermentation of these carbohydrates by colonic bacteria can result in symptoms that are very similar to those experienced in coeliac disease. This reinforces the concept that improvement in gastrointestinal symptoms after exclusion of gluten from the diet cannot be relied on as a diagnostic tool in the evaluation of potential coeliac disease.
The symptoms of coeliac disease vary markedly from person to person, and up to 50% of people are asymptomatic. While coeliac disease has traditionally been thought of as a condition of malnutrition and wasting, it is clear that the epidemiology has changed. In population studies, people with coeliac disease could not be identified by their weight or symptoms.3,4 Clinical features, if present, can include:
There are associated conditions which increase the risk of the patient having coeliac disease. The clinician should have a high index of suspicion for coeliac disease if the patient has:
Many patients are asymptomatic or have very few symptoms and thus a high index of suspicion is required. Those with any symptoms suggestive of coeliac disease should be tested. Asymptomatic people who are first-degree relatives of those diagnosed or who have any of the associated conditions should be screened with serological testing.5
If serology is negative, but there is a high index of suspicion, further testing should be performed. If serology is positive the diagnosis is confirmed by endoscopy with small bowel biopsy (see Fig.).
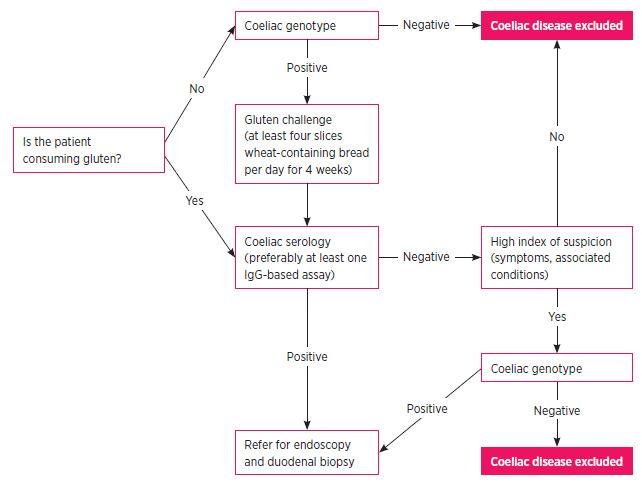
Serological testing for coeliac disease requires the patient to be consuming a diet containing gluten at the time of testing. Before testing it is therefore important to clarify dietary gluten consumption. If the person being tested has limited or no gluten consumption then there needs to be a ‘gluten challenge’ with at least four slices of wheat-containing bread per day for at least four weeks before testing. Patients undertaking a gluten challenge commonly experience some gastrointestinal symptoms but these symptoms are often short lived (often limited to 2–3 days). Importantly, the development of symptoms in response to the gluten challenge is insufficient and inaccurate in diagnosing coeliac disease. Conversely, relief of symptoms in response to a gluten-free diet has no role in diagnosis. If there are patient concerns about gastrointestinal symptoms that will develop due to a gluten challenge, suggesting a gluten-containing product with less fermentable sugars (such as spelt flour-based breads) can help reduce the symptoms.
Most serological screening tests for coeliac disease use either IgA or IgG antibodies. Many Australian laboratories test for both an IgA and IgG coeliac specific antibody (see Table).2,6 This is important, because approximately 3–5% of patients with coeliac disease have IgA deficiency so testing for an IgA coeliac specific antibody alone would be unreliable in these patients.1 Many laboratories therefore also measure total IgA to aid in interpretation. In addition, IgA coeliac antibody testing is unreliable in children less than four years of age due to immaturity of the immune system.
Antibody testing has a high sensitivity and specificity. However, false negative and false positive tests occur in approximately 5% of tests. The prevalence of seronegative coeliac disease is estimated at up to 5% of those diagnosed.7
The Australian Coeliac Society has produced recommendations on the use of genotype testing in coeliac disease.8 The greatest value in testing for the HLA-DQ2/DQ8 haplotype is to exclude coeliac disease. More than 99% of patients with coeliac disease will test positive for HLA-DQ2/DQ8, thus a negative test effectively excludes coeliac disease. A positive test is not helpful in diagnosing coeliac disease as 30–50% of the population carry the genes and only 10% of people who test positive will actually have coeliac disease.9
A specific scenario where genotype testing can be helpful is in the patient who has already commenced a gluten-free diet. If the genotype testing is negative, then coeliac disease can be confidently excluded, whereas a positive test indicates the need for formal testing after a gluten challenge.
Genotype testing can also be helpful to exclude coeliac disease when the diagnosis of coeliac disease is in doubt, such as when small bowel histology or coeliac antibody testing is equivocal. A positive genotype test in the setting of a negative small bowel biopsy and negative serology on a gluten-containing diet indicates that the patient has a genetic susceptibility but no current coeliac disease.9
Prescribing a gluten-free diet should not be taken lightly. The diet is expensive, socially isolating and there is some evidence that questions the nutritional adequacy of a gluten-free diet when used in conditions other than coeliac disease. Given the false–positive rate with serology, commencing a strict life-long gluten-free diet is not recommended without a definite diagnosis of coeliac disease. A gastroscopy for small bowel (duodenal) biopsy is the gold standard and is recommended for all patients to confirm the diagnosis. It is generally a well-tolerated procedure with few risks.
Adults with elevated coeliac antibodies should be referred for endoscopy. Patients with normal concentrations of antibodies but in whom there is a high clinical suspicion of coeliac disease should also be referred for endoscopic evaluation. As with coeliac antibodies, the specific changes associated with coeliac disease will only be present on histology if the patient is consuming a gluten-containing diet.
Histology of the small bowel in untreated coeliac disease shows intraepithelial lymphocytosis and villous atrophy of varying severity. Other causes of intraepithelial lymphocytosis and villous atrophy on small bowel biopsies include infectious gastroenteritis, giardiasis, Crohn’s disease, tropical sprue, and use of non-steroidal anti inflammatory drugs.
In children, the European Society for Paediatric Gastroenterology, Hepatology and Nutrition has proposed that a tissue diagnosis can be avoided in specific circumstances. These are when there are signs and symptoms of coeliac disease and a high titre of coeliac specific antibodies (10 times the upper limit of normal) and an at-risk genotype (HLA-DQ2/DQ8 haplotype). This proposal is controversial and we still recommend referral to a paediatric gastroenterologist before starting a gluten-free diet in these children.
Screen and treat nutrient deficiencies and other complications:
In addition to clinical assessment and checking the resolution of symptoms, tests are used for assessing the response to a gluten-free diet:
Coeliac disease is an immune-mediated condition causing small bowel mucosal damage in genetically susceptible individuals exposed to gluten derived from wheat, rye and barley. Most tests for coeliac disease require the patient to be consuming a gluten-containing diet at the time of testing.
Although genotype testing can be performed on a gluten-free diet, it is most useful in excluding rather than confirming the diagnosis of coeliac disease. Importantly, a symptomatic response to a gluten challenge or withdrawal of gluten from the diet is insufficient and inaccurate for a diagnosis. A tissue diagnosis from duodenal histology obtained at the time of gastroscopy remains the gold standard for diagnosing coeliac disease.
Conflict of interest: none declared

Gastroenterologist, Eastern Health, Melbourne
Gastroenterology advanced trainee, Eastern Health, Melbourne
Gastroenterologist and Director of General Medicine, Eastern Health, Melbourne
Researcher, Eastern Health Clinical School, Monash University, Melbourne
